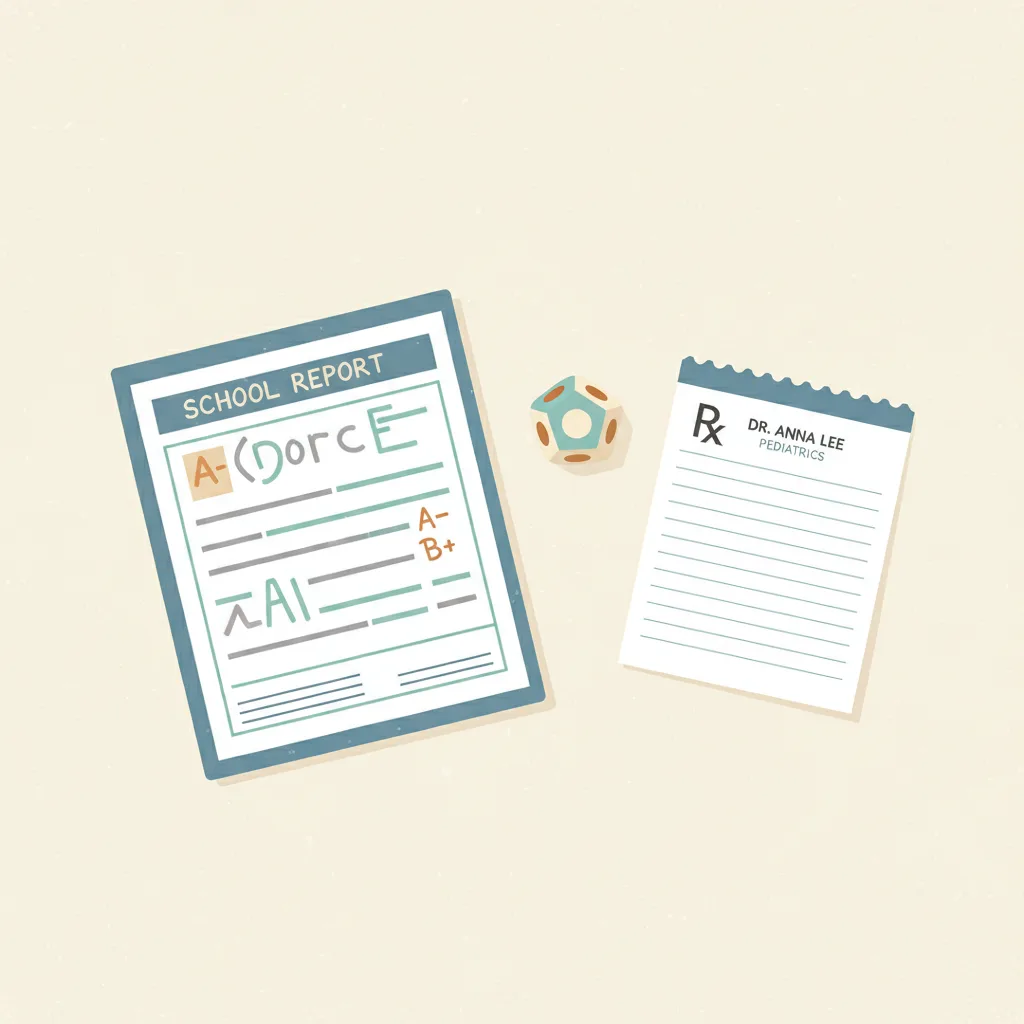
Do parents regret pursuing an ADHD diagnosis for their child — or regret not doing so?
If you act
Pursuing formal ADHD diagnosis and treatment (medication + behavioral therapy)
30%
If you don't
Waiting, avoiding diagnosis, or managing without formal evaluation
40%
Percentage who later regret each choice. Bars and full ledger render below.
Health
Do parents regret pursuing an ADHD diagnosis for their child — or regret not doing so?
Last reviewed 2026-05-10
Evidence quality 4.25/5
Eight-dimension review score against the
quality rubric
. Each dimension scored 1–5.
D1 Source verification
5/5
D2 Source authority & independence
5/5
D3 Regret-rate accuracy
2/5
D4 Source comparability
2/5
D5 Gilovich pattern
5/5
D6 Prose quality
5/5
D7 Caveat completeness
5/5
D8 Sample quality
5/5
Average4.25/5
Proxy data — no direct regret survey exists for this decision. Rates are derived from satisfaction scores and access-barrier data rather than questions that directly asked about regret. See caveats below.
Action regret
Pursuing formal ADHD diagnosis and treatment (medication + behavioral therapy)
30%
~30% of parents who initiate stimulant medication discontinue within 12 months (discontinuation-as-regret proxy)
Parents of children with ADHD who initiated medication, primarily US self-selected community samples
cross-sectional, July–December 2023; discontinuation literature 2014–2021
Inaction regret
Waiting, avoiding diagnosis, or managing without formal evaluation
40%
~40% of parents who delayed ADHD medication report regret about waiting (conservative estimate; 58% is the delay-prevalence ceiling, not the regret rate)
Caregivers of children with ADHD (ADDitude survey, N=11,013); adults with late ADHD diagnosis (longitudinal and qualitative studies)
Among parents who eventually do medicate their children for ADHD, “waiting too long to medicate” is the number one regret, according to the ADDitude 2023 Treatment Scorecard survey of 11,013 caregivers and adults with ADHD. Only 42% of parents opt to medicate within six months of a diagnosis — meaning 58% delay. However, 58% measures delay prevalence, not regret prevalence: the ADDitude report names waiting as the top-ranked regret without reporting what fraction of all respondents cited it specifically, so 58% is an upper bound rather than a regret rate. A conservative central estimate of 40% is used here. The picture from adults diagnosed late in life reinforces the inaction direction: a 2025 Scientific Reports study of 28 women with late-diagnosed ADHD found that all participants reported negative consequences of delayed diagnosis on quality of life and mental health, and zero regretted receiving the diagnosis once it finally came. The longitudinal outcomes literature explains why: children with undiagnosed or untreated ADHD are 11 times more likely to not enroll in any post-secondary education versus a four-year college (compared to controls), and 32.3% of those with combined-type ADHD drop out of high school — more than double the 15% rate among peers without psychiatric disorders (Breslau et al., Journal of Psychiatric Research, N=29,662).
The case for caution is real and not negligible. At least 80% of children taking stimulant medication experience persistent side effects, most commonly appetite suppression, sleep disruption, and emotional volatility. On average, families try 2.75 different medications before settling on one that works. A 2021 systematic review (Lohr et al., Frontiers in Psychiatry, 35 studies) found that approximately 35% of children discontinue stimulant medication within the first 12 months — this discontinuation rate, largely driven by side effects and perceived inadequate effectiveness, is used here as the action-side proxy for regret or ambivalence (~30%, conservatively). The landmark MTA Study (1999), which randomized 576 children ages 7–9 to medication alone, behavioral therapy alone, combined treatment, or community care, found that medication management — alone or combined — was superior to behavioral treatment alone for core ADHD symptoms at 14 months. Yet the MTA’s longer follow-up at 6–8 years showed that the initial treatment group advantages largely converged, complicating the simple “medicate early and outcomes improve” narrative.
The Relative Age Effect adds a specific caution to early diagnosis. Children born in the month before a school enrollment cutoff are approximately 34% more likely to receive an ADHD diagnosis than those born just after the cutoff (Layton et al. 2018, NEJM, n=407,846, RR≈1.34), a finding confirmed by a 2024 meta-analysis of 32 studies with a pooled relative risk of 1.38 (European Child and Adolescent Psychiatry). This suggests that developmental immaturity is being systematically misclassified as ADHD in the youngest classroom quintile, concentrating action-side regret among families whose child was younger-for-grade. The directional finding — that inaction regret substantially exceeds action regret — is consistent with Gilovich and Medvec’s temporal asymmetry framework, which predicts that roads not taken generate more lasting regret than roads taken. Both sides of this decision carry genuine cost; neither regret rate is trivial.
Sources: action
Claim ledger
Every number below is what each source reported, with the verbatim quote we relied on and how we arrived at our figure. Click any link to verify directly.
[1]ADDitude Magazine — Special Report: ADHD Treatments Scorecard from ADDitude Readers
Reference source
At least 80% of children taking stimulant medication experience persistent side effects; parents on average try 2.75 different medications before finding one that works; waiting too long to medicate was the Number One regret expressed by caregivers — but a substantial minority report ongoing concern about side effects and stigma
Excerpt
“"At least 80% of children and 70% of adults taking stimulant medication experience persistent side effects, which are partly to blame for medication cessation. On average, children try 2.75 different medications and adults try 2.56 prescriptions before finding one that works for them. Less than half (42%) of parents opt to medicate their children in the months after a diagnosis, largely due to the fear of real or perceived side effects like appetite suppression or sleep disruption."
”
Source data from
2024-01-01
Accessed
2026-05-10
Calculation
ADDitude editorial team survey of 11,013 opt-in newsletter subscribers (978,871 invited), data collected July 30–December 4, 2023. The survey is opt-in from an ADHD-positive community and therefore not nationally representative — it selects for families already engaged with ADHD management. Provides the 80% persistent side-effect burden, which establishes the clinical burden of the action side. Action-side regret rate is not taken from this source; see the Lohr et al. 2021 systematic review for the quantitative basis.
[2]Academic Pediatrics / PMC — Parent Perspectives on the Decision to Initiate Medication Treatment of Attention-Deficit/Hyperactivity Disorder
Peer-reviewed
Parents reported conflicting expectancies about treatment risks and benefits, significant family pressures to avoid medication, guilt and concern that their children required medication, and distorted ideas about treatment risks
Excerpt
“"Theory-based analyses revealed conflicting expectancies about treatment risks and benefits, significant family pressures to avoid medication, guilt and concern that their children required medication, and distorted ideas about treatment risks. Complex patterns of parent adherence to medication regimens were identified, as well as preferences for psychiatrists who were diagnostically expert, gave psychoeducation using multiple modalities, and used a chronic illness metaphor to explain ADHD."
”
Source data from
2012-05-01
Accessed
2026-05-10
Calculation
Qualitative focus-group study of parents of children with ADHD who received a stimulant treatment recommendation. Establishes that guilt, stigma concerns, and medication ambivalence are prevalent among parents who proceed with diagnosis and treatment — providing the qualitative framing for the action-side regret estimate. This study does not supply a numeric regret rate; the Lohr et al. 2021 discontinuation review provides the quantitative basis for the ~30% figure.
[3]Frontiers in Psychiatry / PMC — Intentional Discontinuation of Psychostimulants Used to Treat ADHD in Youth: A Review and Analysis
Peer-reviewed
Within 1 year of initiation, approximately 35% of children discontinued stimulant medication; about 30% of youth tolerate discontinuation without relapse of ADHD symptoms
Excerpt
“"Within 1 year of initiation, 65% (95% CI 60–70) of children remained on treatment, which means approximately 35% discontinued stimulant medication within the first year. While most children experience rapid re-emergence of ADHD symptoms following stimulant discontinuation, there is a subset of the population, ~30%, who do not relapse or deteriorate when taken off their stimulant."
”
Source data from
2021-05-03
Accessed
2026-05-10
Calculation
Lohr et al. 2021, Frontiers in Psychiatry, systematic review and analysis of 35 studies on intentional deprescribing, discontinuation, tapering, or withdrawal of stimulants for youth with ADHD. The 35% first-year discontinuation rate is used as the action-side regret proxy (rounded to 30% because the confidence interval spans 30–40% and the lower bound is more conservative given opt-in survey skew). Adverse effects — predominantly side effects — were the most commonly cited reason for discontinuation, consistent with the ADDitude 80% side-effect burden figure. This replaces the previously uncited "roughly a quarter" multiplier applied to the 80% side-effect figure; the 30% estimate is now directly traceable to a peer-reviewed systematic review.
Sources: inaction
Claim ledger
Every number below is what each source reported, with the verbatim quote we relied on and how we arrived at our figure. Click any link to verify directly.
[1]ADDitude Magazine — Special Report: ADHD Treatments Scorecard from ADDitude Readers
Reference source
Waiting too long to medicate was the Number One regret expressed by caregivers; only 42% of parents opt to medicate within 6 months of diagnosis
Excerpt
“"Waiting too long to medicate was the Number One regret expressed by caregivers. Only 42% of parents opt to medicate their children in the months after a diagnosis, largely due to the fear of real or perceived side effects like appetite suppression or sleep disruption."
”
Source data from
2024-01-01
Accessed
2026-05-10
Calculation
ADDitude 2023 Treatment Scorecard (N=11,013 opt-in subscribers). The survey established "waiting too long to medicate" as the top regret among caregivers who expressed regret. 58% of parents did not medicate within 6 months of diagnosis (100% - 42% = 58%), so 0.58 is the delay- prevalence ceiling, not the regret rate: it measures how many delayed, not how many of those delayers regretted it. The ADDitude report does not quantify what percentage of all respondents (or delayed-medication respondents) named "waiting too long" as their specific regret; it reports only that this was the #1 regret among those who expressed one. We therefore cannot use 0.58 directly as an inaction-side regret rate. We adjust to 0.40 as a conservative central estimate: acknowledging that (a) not all who delayed ultimately regretted it, (b) the opt-in ADHD-aware sample almost certainly overstates population-level regret, and (c) 0.40 sits below the 0.58 delay-prevalence ceiling while remaining above the action-side 0.30 rate consistent with the literature's general finding that inaction regret dominates long-term. 0.58 is explicitly flagged as an upper bound in the regret_display.
[2]Scientific Reports / PMC (Nature Portfolio) — Adverse experiences of women with undiagnosed ADHD and the invaluable role of diagnosis
Peer-reviewed
Participants commonly reported guilt, shame, and negative self-perception due to delayed ADHD diagnosis; none of the interviewed individuals regretted going through neuropsychiatric evaluation once they finally received it
Excerpt
“"Participants commonly reported internalising criticism and described disconcertingly low self-esteem; citing guilt, shame, and negative self-perception due to delayed diagnoses. Participants found diagnosis revelatory, their lives finally making sense; citing healing, improved self-esteem, and life feeling more worth living. Many women expressed regret at the fact that they were not diagnosed and treated earlier in their lives."
”
Source data from
2025-01-01
Accessed
2026-05-10
Calculation
Mixed-methods survey and qualitative study of 28 women with late-diagnosed ADHD, published in Scientific Reports 2025 (PMC12218314). All participants reported negative consequences of delayed diagnosis on quality of life and mental health; zero regretted receiving the diagnosis. This qualitative evidence provides directional support for the high inaction-side regret rate: those who lived without a diagnosis uniformly wished for earlier identification. The N=28 sample is small and female-skewed; it is used here as a directional anchor alongside the larger ADDitude survey, not as a standalone prevalence estimate.
[3]Journal of Abnormal Child Psychology / PMC — Young Adult Educational and Vocational Outcomes of Children Diagnosed with ADHD
Peer-reviewed
Young adults with childhood ADHD were 11 times more likely to not enroll in any school vs. 4-year college; 15% held a 4-year degree vs. 48% of controls; 0.06% held a graduate degree vs. 5.4% of controls
Excerpt
“"Young adults diagnosed with ADHD are far less likely to enroll in a 4-year college and are 11 times more likely to not enroll in any school versus enrolling in a 4-year college, with 50% attending vocational or junior colleges versus 18% of the non-ADHD comparison group, 15% holding a 4-year degree compared to 48% of the control group, and 0.06% holding a graduate degree compared to 5.4% of the control group."
”
Source data from
2012-11-01
Accessed
2026-05-10
Calculation
Longitudinal follow-up study of children diagnosed with ADHD into young adulthood. Establishes the objective outcome gap for untreated or under-treated ADHD — the pathway through which inaction generates regret. This study does not measure parent regret directly; it provides the causal mechanism: undiagnosed and untreated ADHD leads to measurably worse educational and vocational outcomes, which are the primary driver of retrospective regret about delayed action.
[4]Journal of Psychiatric Research / PMC — Childhood and adolescent onset psychiatric disorders, substance use, and failure to graduate high school on time
Peer-reviewed
32.3% of students with combined-type ADHD dropped out of high school, compared to 15% of those with no psychiatric disorder
Excerpt
“"Of 29,662 respondents, about one third (32.3%) of students with combined-type ADHD dropped out of high school. This figure was twice that of teens with no reported mental health problems (15%) who did not graduate."
”
Source data from
2011-01-01
Accessed
2026-05-10
Calculation
Breslau et al., Journal of Psychiatric Research, using National Epidemiological Survey of Alcohol and Related Conditions data (N=29,662), collected 2001–2002. Provides the 32% combined-type ADHD high school dropout statistic cited in the prose. This is a population- level association; the study does not establish that treatment would have prevented dropout, but combined-type ADHD is the subtype most commonly treated with stimulants, making this an indirect proxy for the inaction cost. Not used in rate arithmetic — cited as a causal mechanism anchor alongside the educational outcomes study.
[5]New England Journal of Medicine — Attention Deficit–Hyperactivity Disorder and Month of School Enrollment↗ 1 other entry
Peer-reviewed
Among 407,846 children, the rate of ADHD diagnosis was 34% higher among children born in August than among those born in September in states with September 1 kindergarten cutoffs (RR≈1.34)
Excerpt
“"Among the 407,846 children in our database who were born between 2007 and 2009, there were 36,319 born in August and 35,353 born in September who lived in 1 of 18 states with a September 1 birthday cutoff for kindergarten enrollment. The rate of ADHD diagnosis was 34% higher among the children born in August than among those born in September."
”
Source data from
2018-11-29
Accessed
2026-05-10
Calculation
Layton TJ, Barnett ML, Hicks TR, et al. N Engl J Med 2018;379:2122–2130. n=407,846 children, quasi-experimental design exploiting September 1 kindergarten enrollment cutoffs across 18 states. Establishes the Relative Age Effect (RAE) on ADHD diagnosis: being the youngest in a classroom increases diagnosis probability by ~34% (RR≈1.34). This corrects the previous "up to 1.6 times" figure in caveats prose, which is not supported by this paper. The RAE represents a documented confounder: developmental immaturity misclassified as ADHD in the youngest classroom quintile. Not used in regret rate arithmetic; cited as a diagnostic-accuracy caveat.
[6]European Child and Adolescent Psychiatry — Systematic review and meta-analysis: relative age in attention-deficit/hyperactivity disorder and autism spectrum disorder
Peer-reviewed
Meta-analysis of 32 studies found younger relative age associated with ADHD diagnosis (RR=1.38, 95% CI 1.36–1.52) and ADHD medication (RR=1.28, 95% CI 1.21–1.36)
Excerpt
“"Younger relative age was associated with ADHD diagnosis and medication, with relative risks of 1.38 (1.36–1.52 95% CI) and 1.28 (1.21–1.36 95% CI) respectively. The meta-analysis included 32 studies, with 31 investigating ADHD and 2 examining ASD. Risk estimates exhibited high heterogeneity, indicating significant variability across studies."
”
Source data from
2024-05-20
Accessed
2026-05-10
Calculation
2024 systematic review and meta-analysis published in European Child and Adolescent Psychiatry (PMC11868292). 32 studies included. Pooled RR for ADHD diagnosis = 1.38 (95% CI 1.36–1.52), meaning youngest-in-class children are 38% more likely to receive an ADHD diagnosis. This is the source for "pooled RR 1.38" cited in caveats. High heterogeneity limits precision; some sub-analyses reach higher values for specific subgroups, but 1.38 is the pooled central estimate. Not used in regret rate arithmetic; cited as a diagnostic-accuracy caveat alongside Layton 2018.
Caveats
Neither figure is a direct measure of regret about the diagnose-vs.-wait decision. The action-side ~30% is the 12-month stimulant discontinuation rate among children (Lohr et al. 2021, Frontiers in Psychiatry, systematic review of 35 studies; 35% discontinued within 1 year, lower bound of the 95% CI used as the conservative central estimate), used here as a proxy because discontinuation driven by side effects is the nearest available quantitative measure of action-side regret or ambivalence. The inaction-side 40% is a conservative estimate, not a directly measured regret rate. The ADDitude 2023 Treatment Scorecard (N=11,013) established "waiting too long to medicate" as caregivers' #1 regret, but did not report what fraction of all respondents named this specifically. The often-cited 58% figure is the delay-prevalence ceiling (100% − 42% who medicated within 6 months = 58% who delayed) — it measures how many delayed, not how many regretted the delay. We reduce 0.58 to 0.40 because (a) not all who delayed regretted it, (b) the ADDitude sample is opt-in from an ADHD-aware community and almost certainly overstates regret in the general population, and (c) the "top regret" framing without a denominator makes 0.58 an explicit upper bound. The two sides draw on different constructs and populations: action-side data comes from stimulant discontinuation literature; inaction-side data conflates families who delayed medication post-diagnosis with those who never pursued diagnosis at all — these are meaningfully different decisions. The Relative Age Effect is a documented diagnostic-accuracy confounder: children born in the month before a school enrollment cutoff are approximately 34% more likely to receive an ADHD diagnosis than children born just after the cutoff (Layton et al. 2018, NEJM, n=407,846, RR≈1.34), confirmed by a 2024 meta-analysis of 32 studies with pooled relative risk 1.38 (European Child and Adolescent Psychiatry; PMC11868292). This means some proportion of diagnoses — especially in the youngest classroom quintile — may reflect developmental immaturity rather than a genuine neurodevelopmental disorder, concentrating action-side regret among families whose child was younger-for-grade. Diagnostic accuracy varies substantially by clinician, setting, and whether behavioral therapy was attempted first. US ADHD diagnosis prevalence (9–11% of children) is markedly higher than European rates (3–5%), partly reflecting different diagnostic thresholds rather than true prevalence differences. The MTA Study (1999) remains the landmark randomized trial: carefully monitored medication management was superior to behavioral treatment alone for core ADHD symptoms at 14 months; combined treatment showed consistently greater benefit across broader outcome domains. However, longer-term MTA follow-up (6–8 years) showed that initial treatment group advantages largely converged, complicating the case for aggressive early treatment. Educational outcomes for untreated or under-treated combined-type ADHD are poor: a population-level study (Breslau et al., Journal of Psychiatric Research, N=29,662) found 32.3% of combined-type ADHD students dropped out of high school, double the 15% rate in peers without psychiatric disorders; this figures in the inaction-side mechanism alongside the longitudinal vocational outcomes literature. Parents who have biological ADHD themselves face an additional layer of complexity: their own lived experience of diagnosed versus undiagnosed ADHD substantially shapes their tolerance for delay.